Why Infection Preventionists Must Expand Surveillance Beyond Traditional Targets
By: Amanda Taylor & Jill Holdsworth
Infection preventionists are trained to think broadly during an outbreak. We trace exposures, evaluate workflows, identify environmental risks, assess adherence to transmission-based precautions, and look for patterns that others may miss. Yet even with increasingly sophisticated surveillance programs, areas of healthcare often remain underrecognized during outbreak investigations.
As healthcare systems continue responding to emerging infectious threats such as Ebola Virus Disease, Measles, and Hantavirus Pulmonary Syndrome, infection preventionists are being asked to think beyond traditional outbreak pathways. Portable imaging devices, shared equipment, procedural ultrasound use, and gaps in traceability create vulnerabilities that may not appear on standard surveillance dashboards — but can become critically important during an outbreak response. The reality is simple: ultrasound touches far more patients than most organizations realize, yet it is rarely included in routine infection surveillance or outbreak preparedness planning.
During an outbreak investigation, infection preventionists focus on identifying where transmission may have occurred. The challenge is that outbreaks rarely expose only one failure. Instead, they reveal system vulnerabilities that had existed quietly for months or even years. In recent years, healthcare facilities have faced increasing scrutiny regarding preparedness for emerging infectious diseases. Highly communicable pathogens force organizations to rapidly evaluate shared equipment workflows, cleaning and disinfection practices, staff competency, PPE compliance, and environmental contamination risks, among other areas.
While many organizations focus heavily on rooms, isolation protocols, and reusable surgical instrumentation during preparedness planning, ultrasound equipment often receives far less attention despite its widespread use across the continuum of care. These devices move rapidly between patients, departments, and levels of care. During an outbreak, that mobility becomes significant.
One of the greatest challenges in outbreak response is identifying shared exposures quickly enough to prevent additional transmission. Portable ultrasound systems introduce unique concerns because they frequently travel throughout facilities while interacting with multiple healthcare workers and patients in high-acuity environments.
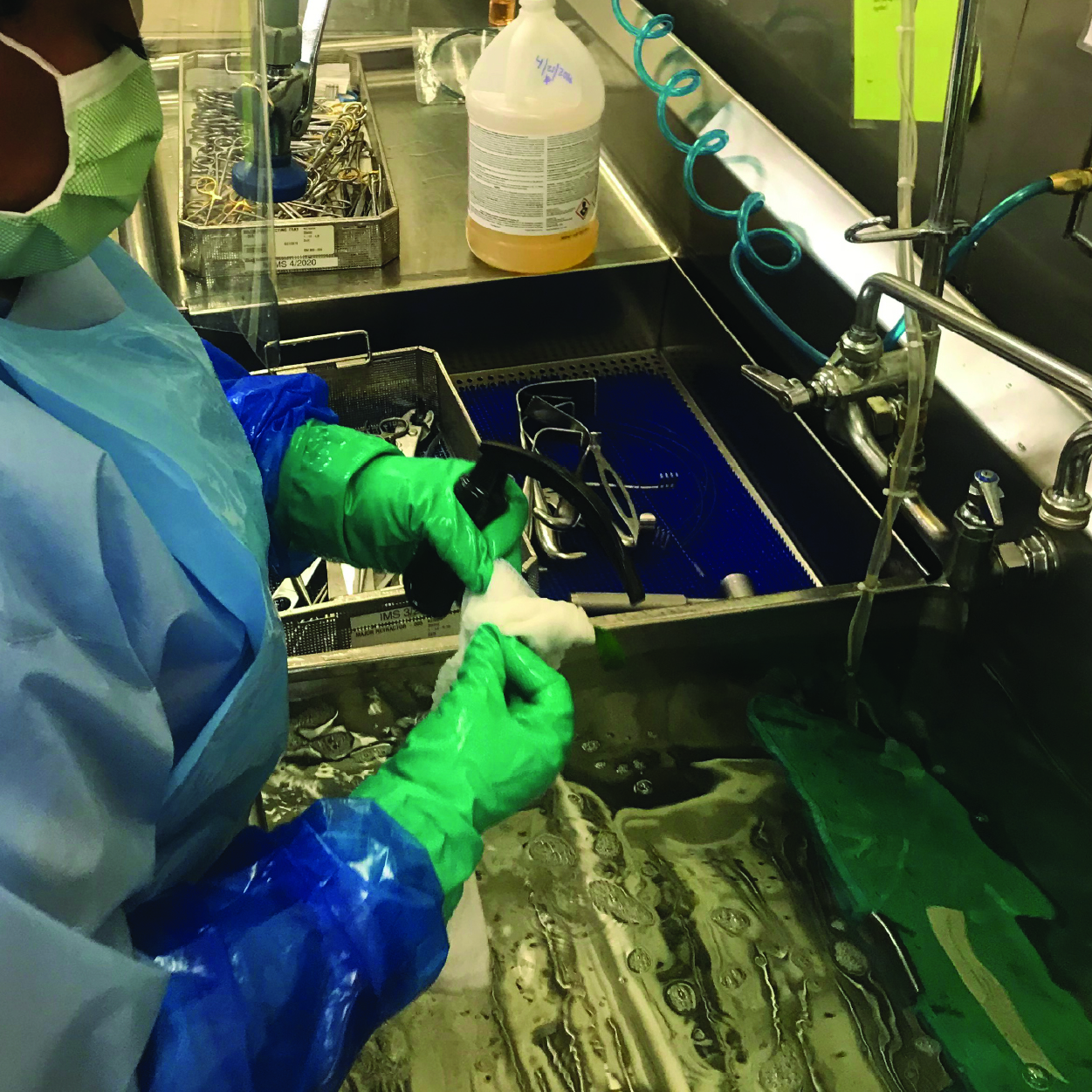
Unlike many reusable medical devices that remain centralized within sterile processing departments, ultrasound probes are often reprocessed in decentralized clinical environments where workflows vary significantly between departments and shifts.
Many infection surveillance programs are largely reactive and outcome-driven. They focus heavily on areas such as SSI (Surgical Site Infections), CLABSI (Central Line-Associated Bloodstream Infections), CAUTI (Catheter-Associated Urinary Tract Infections), VAE (Ventilator-Associated Events), MDRO (Multidrug-Resistant Organisms), PPE (Personal Protective Equipment), and hand hygiene compliance, as well as environmental cleaning metrics.
However, procedures involving ultrasound frequently fall into a surveillance gray zone unless a significant event occurs. This creates a dangerous blind spot.
Traceability has become one of the most important components of modern infection prevention programs. In sterile processing, instrument tracking systems are increasingly expected. However, ultrasound probe traceability remains inconsistent across healthcare settings. Since its movement is rarely captured in the EHR (Electronic Health Record), the device becomes an invisible, untraceable vector silently moving throughout the facility. Under-tracked ultrasound equipment essentially functions as a “ghost fomite”, serving as a hidden source for organism transmission.
Without accurate traceability, outbreak investigations become exponentially more difficult. Manual documentation processes often make this nearly impossible, and during an outbreak, an IP’s greatest asset is time. Without automated traceability, determining exactly which patients came into contact with a specific probe or console would be a highly difficult, time-consuming process that would likely lead to an underestimated calculation of risk. If ultrasound traceability is integrated directly into an organization’s electronic surveillance system, the investigation shifts instantly. Instead of manually pulling paper logs from various departments to see who used a specific probe, electronic surveillance data can automatically populate a map showing the machine's locations and a list of all patients it was used on./p>
To effectively move ultrasound out of the surveillance gray zone, infection prevention programs must shift their surveillance from solely tracking infections to also tracking process vulnerabilities. Infection preventionists should conduct active surveillance of portable ultrasound machines, tracing a single machine throughout an entire shift. This process tracks the device across departments, hand hygiene compliance, and machine disinfection between patient rooms, not just at the end of the day.
Specific, quantifiable ultrasound metrics should be added to surveillance dashboards. Monthly counts of ultrasound exams performed in decentralized environments (Emergency Department, clinic exam rooms) versus centralized areas (radiology) could be monitored to identify high-velocity, high-risk departments that require more auditing activities and resources. A high percentage of ultrasound procedures in which the unique device ID lacks a corresponding electronic reprocessing log entry can signal a failure in the workflow chain in which a probe was used, and its disinfection status was not recorded. No matter the metrics chosen, it is clear that adding ultrasound metrics to surveillance programs is needed to strengthen outbreak preparedness and response.
Automated documentation and electronic traceability systems can significantly strengthen outbreak preparedness. Ultrasound should be incorporated into surveillance systems long before a cluster or outbreak is identified. That means investing in clear, risk-based policies, standardizing disinfection and traceability processes, validating staff competency, and conducting routine audits across all settings where ultrasound is used. These are core data elements that will help facilities quickly identify a common source to prevent further transmission. From an infection prevention perspective, this is not simply a workflow convenience — it is a patient safety necessity.
The future of outbreak preparedness will require broader thinking from healthcare organizations. Infection preventionists are increasingly being asked to evaluate not only whether policies exist, but whether systems are truly resilient under stress. Healthcare facilities have spent years strengthening oversight of sterile processing, instrument traceability, and environmental cleaning programs. Ultrasound reprocessing deserves the same level of attention. By treating ultrasound equipment as a critical variable in surveillance, healthcare organizations can move away from post-outbreak damage control towards true, proactive infection prevention. When an outbreak occurs, the greatest risk is often not the process everyone is watching closely—it is the one no one thought to include.
Guest Author, Amanda Taylor is the System Director of Epidemiology and Central Surveillance at Appalachian Regional Healthcare (ARH), where she leads system-wide infection prevention initiatives and oversees centralized surveillance programs across the health system. With extensive experience in healthcare epidemiology, Amanda developed ARH’s first centralized surveillance program and has played a key role in advancing infection prevention strategies, healthcare construction risk management, and disease surveillance. Her expertise focuses on improving patient safety through evidence-based practices, standardized processes, and data-driven quality improvement across acute care and ambulatory settings.
*Disclaimer: The information shared in this article is that of the author(s) and should be reviewed by the consumer as that written by an independent party to CS Medical or in conjunction with CS Medical staff. The article may or may not directly represent any employer, company, or third party, and are solely that of the individual(s) or contributors themselves.