Reprocessing medical devices is crucial to patient safety and the prevention of healthcare-associated infections (HAIs). A study by The Joint Commission in 2016 found that 74 percent of all immediate threat to life declarations were associated with the improper equipment sterilization or high-level disinfection.1 Similarly, performance of intermediate and high-level disinfection and sterilization of medical equipment, devices, and supplies (IC.02.02.01, EP 2) was recorded as an area with the highest non-compliance amongst facilities surveyed in 2022.2 In addition, a survey of infection preventionists in the US found that 20% of respondents were aware of a time that a probe used in a procedure was incorrectly processed.3 This response rate likely represents an underestimate because deviations from the reprocessing procedure may go unnoticed. Together, these findings suggest that many facilities continue to struggle with proper medical device reprocessing.
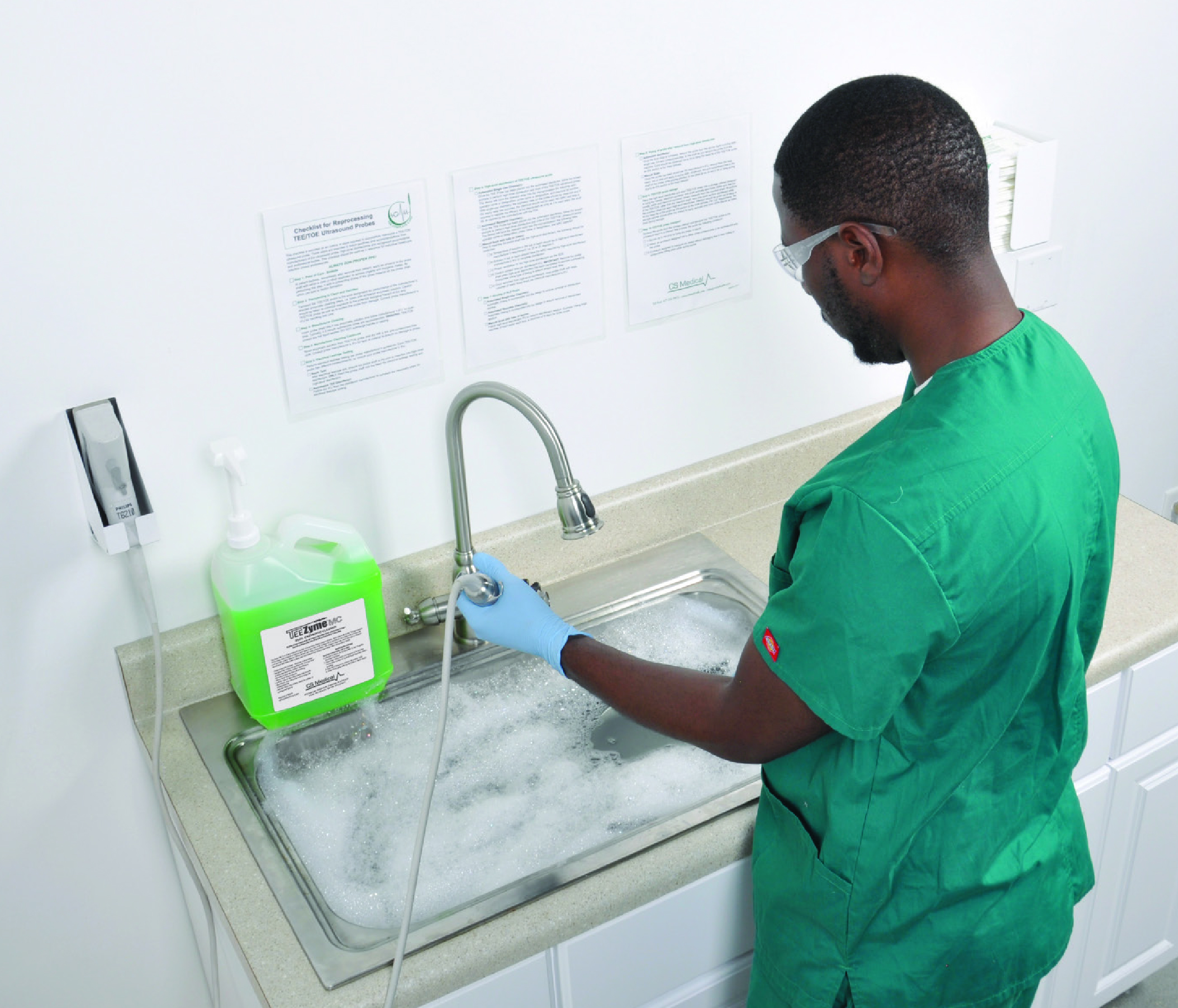
Manual cleaning of a transvaginal probe using an enzymatic cleaner per manufacturer’s recommendation
Proper medical device reprocessing requires a balance between the time and resources required to complete the procedure and the risk of HAIs and probe damage. Most professional and regulatory agencies recommend that facilities use the Spaulding classification to determine how to reprocess medical devices. This classification system divides medical devices into three categories: non-critical, semi-critical, and critical devices (Table 1). Using this classification system, non-critical devices should be low or intermediate level disinfected, semi-critical devices should be high-level disinfected, and critical devices should be sterilized.4-8 According to the Spaulding classification, transvaginal and transrectal ultrasound probes are considered semi-critical devices and must be cleaned and high-level disinfected prior to use.4-8 Importantly, the use of a procedure cover does not change the Spaulding classification of a medical device.4,5 High-level disinfection (HLD) is a process that eliminates all microorganisms from a device, except for small numbers of bacterial spores. HLD of transvaginal and transrectal ultrasound probes, as well as other medical devices, is no small feat. However, innovations in the last two decades have improved the available transvaginal and transrectal probe reprocessing methods from manual and semi-automated (manual cleaning and automated disinfection) to completely automated procedures.
Table 1. Spaulding classification of medical devices.
| Classification | Definition | Recommended reprocessing |
|---|---|---|
| Non-critical | Devices used on intact skin | Cleaning and low- or intermediate-level disinfection |
| Semi-critical | Devices that come in contact with mucous membranes or non-intact skin | Cleaning and high-level disinfection |
| Critical | Devices that come in contact with sterile body sites | Cleaning and sterilization |
Traditional reprocessing has utilized manual cleaning and HLD procedures. In these methods, the transvaginal or transrectal probe is processed at the point-of-use then cleaned and high-level disinfected by submersion in a compatible cleaner and high-level disinfectant, respectively. While these methods do not require specialized equipment, they can be tedious. Each probe must be inspected and reprocessed individually and correctly using a detailed, multi-step procedure that may vary between probe models; potentially resulting in confusion and an increase in human errors. Human error is a significant drawback for any manual procedure. Missteps during the reprocessing procedure can result in ineffective reprocessing putting patients at increased risk of infection and increasing the likelihood of ultrasound probe damage.
Manual soaking station used to high-level disinfect transvaginal and transrectal probes
In addition to being tedious, manual reprocessing procedures are more time-consuming than their automated counterparts. Using the procedures outlined in recognized standards, it is estimated that the total reprocessing time, or the time required to reprocess a probe from point-of-use to storage and hand washing is approximately 48-88 minutes. This timeline is heavily dependent upon the contact time required for the high-level disinfectant. Longer reprocessing times can result in fewer probes available for procedures or require the facilities to purchase additional probes to compensate for longer reprocessing times (Table 2). The manual nature of these methods requires that staff must dedicate the entirety of the lengthy reprocessing time to cleaning and disinfecting a single probe, with little time to complete other clinical duties. Together, these factors may result in pressure on technicians to skip steps to decrease reprocessing times.
Table 2. Estimated maximum number of probes reprocessed in an 8-hour workday per current standards and guidelines
| Method | Manual | Automated |
|---|---|---|
| Number of probes | 10 | 17 |
*Calculated from fastest estimated total reprocessing time assuming 100% efficiency
Long and tedious manual reprocessing procedures have led to the development of automated disinfectors, which are FDA cleared devices that high-level disinfect ultrasound probes using automated methods. Automated disinfectors can decrease the total reprocessing time as much as 61 minutes. As well as the total operator hands-on time or the time that technicians or clinical staff must spend actively engaged in the reprocessing procedure (estimated 27-35 minutes). However, these procedures still require manual cleaning methods and may depend upon manual testing of the disinfectant concentration. Manual cleaning procedures require dedicated time from the operator to complete and are subject to human error. Further, it can be difficult to clean cracks and crevices using manual cleaning methods; resulting in an improperly cleaned device and suboptimal conditions for high-level disinfection.5,10,11
The potential for human error associated with manual methods has resulted in recommendations to use automated methods over manual procedures.1 Greater than 90% of infection preventionists prefer automated ultrasound reprocessing procedures over manual processes.3 Similarly, a survey found that staff feel that automated reprocessing procedures are safer than their manual counterparts.9 However, until recently, there were no options for fully automated reprocessing systems for transvaginal and transrectal ultrasound probes. FDA clearance of the CS Medical Ethos® Automated Cleaner Disinfector in 2023 provided the field with the first automated device to clean and disinfect transvaginal and transrectal ultrasound probes in a single cycle. With a total cycle time of 18 minutes, technicians and clinical staff can clean and disinfect probes quickly so they are ready for the next procedure. The automated nature can reduce human errors and the operator hands-on time required for reprocessing to an estimated 9-20 minutes (Figure 1). This leaves at least 18 minutes of each reprocessing cycle available for other clinical responsibilities to maximize staff and technician time. A fully automated reprocessor provides a reliable and repeatable outcome each time and ultimately gives time back to the healthcare professional to perform other critical tasks, like patient care.
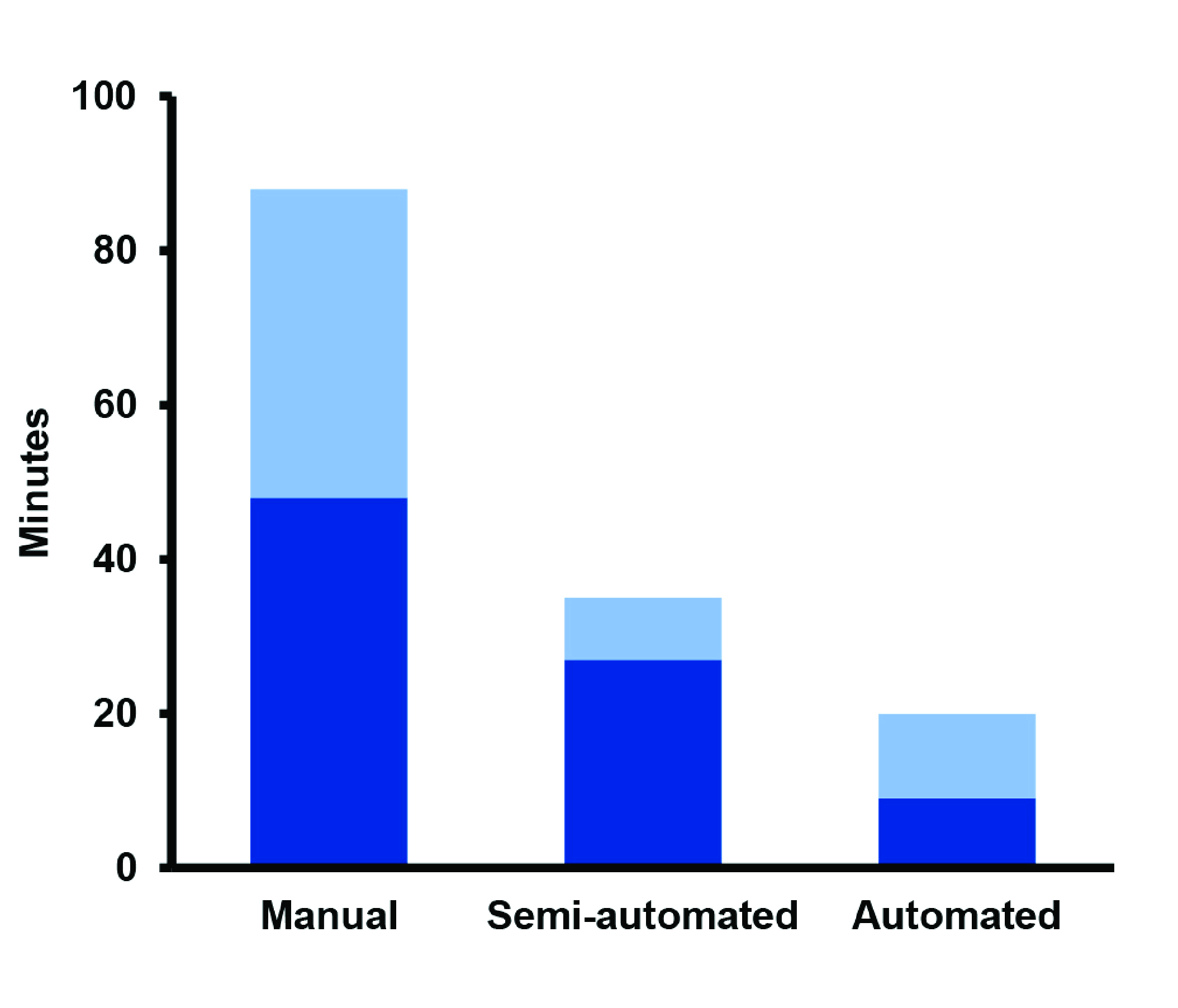
Figure 1. Operator hands-on time required to reprocess one transvaginal probe. Operator hands-on times: Manual, 48-88 min; Automated, 9-20 min. Light blue shows difference between minimum and maximum estimated hands-on time.
Over the last two decades, innovation and technological advances have led transvaginal and transrectal ultrasound probe reprocessing methods from manual to completely automated procedures. These changes in methods have also driven changes in regulations and guidance. While there are more options for transvaginal and transrectal probe reprocessing than ever before, fully automated methods offer numerous advantages. A quick, simple, and efficient workflow can help facilities promote patient safety and prevent HAIs from incorrectly reprocessed ultrasound probes.
Improve Workflows and Reduce Risk with Ethos
Cleaning and disinfecting a transvaginal or transrectal probe with CS Medical’s Ethos Automated Cleaner Disinfector and AquaCide cleaner disinfectant provides a simple, repeatable workflow. Following a procedure, probes are processed at the point of use and cleaned and disinfected using the Ethos Automated Ultrasound Probe Cleaner Disinfector (hereafter, Ethos). Once the cycle is complete, the probe is dried and stored to avoid probe contamination. Relevant procedure details are recorded and stored by Ethos to facilitate documentation using paper or electronic records systems

Simplified workflow with direct placement of ultrasound probe into Ethos using AquaCide® Cleaner Disinfectant — same process each time!
Definitions and abbreviations
Automated cleaner disinfector – an FDA-cleared medical device that has been cleared for use to clean and disinfect medical devices using an automated process. For the purposes of this document, automated cleaner disinfector refers to an FDA-cleared medical device cleared for the cleaning and high-level disinfection of semi-critical transvaginal ultrasound probes.
Chemical indicator – a substance that undergoes an observable change (usually color) when exposed to a threshold concentration of a chemical or active ingredient to determine if minimum recommended concentration is achieved.
Cleaning – the process of removing soil, debris, and foreign materials from medical devices
High-level disinfection (HLD) – most commonly defined as the elimination of all microorganisms on a device or instrument, except for small numbers of bacterial spores
High-level disinfectant – a chemical (usually in liquid, foam, or gaseous form) that kills all microorganisms on a device or instrument, except for a small number of bacterial spores when used according to the manufacturer’s instructions for contact time, temperature, etc.
Low-level disinfection (LLD) – a disinfection process that eliminates all vegetative bacteria (except tubercle bacilli) and most viruses from a device or instrument. Low-level disinfection does not eliminate bacterial spores.
Low-level disinfectant - a chemical (usually in liquid, foam, or gaseous form) that eliminates all vegetative bacteria (except tubercle bacilli) and most viruses from a device or instrument when used according to the manufacturer’s instructions for contact time, temperature, etc.
Minimum recommended concentration (MRC) – the lowest concentration of a chemical or active ingredient at which the disinfectant has been demonstrated to be effective.
Personal protective equipment (PPE) – equipment that is worn by an individual to minimize their exposure to workplace hazards such as hazardous chemicals/disinfectants and microorganisms.
Point-of-use cleaning – a cleaning process performed immediately after use to remove large amounts of gross soil and debris. This process is also sometimes referred to as pre-cleaning.
Probe storage cover – a sleeve designed to cover high-level disinfected probes during storage to protect them from environmental contamination. These sleeves are not designed to be used during ultrasound or medical procedures.
Probe transport vessel– a vessel (ex. bag) that is used to transport soiled probes from the point of care to the appropriate reprocessing area. These vessels should be marked as biohazardous when being used for soiled probes.
Standard operating procedure (SOP) – clear step-by-step instructions for carrying out a specific routine process in a facility or organization. SOPs are important for consistency and quality across multiple operators or departments.
Total estimated reprocessing time – time required to reprocess a probe from point-of-use processing to the final hand hygiene step following probe storage and documentation.
Total operator hands-on time - time that reprocessing technicians or clinical staff must spend actively engaged in the reprocessing procedure.
Transducer procedure cover – a cover, sheath, or condom that is used during ultrasound procedures to provide a physical barrier between the transducer and the tissue to help reduce probe contamination. Transducer procedure covers can fail (tear or be punctured) and should not be used as the only line of defense against cross-contamination. Use of a procedure cover does not change the Spaulding classification of a device.
Recommended equipment list
| Ethos® Automated Ultrasound Probe Cleaner Disinfector | |
| AquaCide® Cleaner High-level Disinfectant | |
| Clean, low-lint (Gamma-irradiated) drying cloth (following disinfection) | |
| Hand soap | |
| Hand washing sink | |
| Log book or electronic reprocessing record system | |
| Low-level disinfectant wipes for cleaning cords and connectors that cannot be subjected to automated disinfection | |
| Personal protective equipment (PPE) (eye protection, gloves) | |
| Probe transport bag | |
| Stickers to label high-level disinfected probes for storage (optional) | |
| Storage cabinet with high efficiency particulate (HEPA)-filtered air (optional) | |
| Transport vessel/bag with biohazard label(s) | |
| Wipe/sponge/cloth for point-of-use cleaning |
Procedure
1. Point-of-Use Processing:
Don the proper personal protective equipment (PPE) including gloves and eye protection to protect from exposure to pathogens on the contaminated probe.5,6 Disconnect the probe from the console and inspect and remove the transducer cover taking care to avoid further contaminating the transducer with blood or bodily fluids.4,6,7 Once removed, the transducer cover should be discarded as biohazardous waste. Wipe the probe with a low-level disinfectant wipe or simple wipe to complete point-of-use cleaning. Minimize delays between use and reprocessing to prevent microbial growth.2 Reprocessing should begin within one hour of point-of-use cleaning.2. Transport:
The Centers for Disease Control and Prevention (CDC) recommends reprocessing be completed in a central reprocessing location.5 However, probes may be reprocessed with Ethos at the point of care because it is a closed automated system that minimizes the release of fumes from the disinfectant/cleaner. If transport to a designated reprocessing area is needed, place the point-of-use processed probe in a designated, clean transport vessel (ex. bag) labeled as biohazardous materials and deliver to the reprocessing area.4,11 Personnel should remove and discard their gloves in the biohazardous waste and wash their hands after handling the probe to prevent the spread of potentially pathogenic microorganisms from the contaminated probe.7
Transporting a soiled transvaginal probe though the healthcare system.
3. Cleaning and High-level Disinfection (HLD) Setup:
Check that the Ethos is ready for use. If the Ethos is off, flip the power switch to “on” and wait for the system to startup. Remove the probe from the transport vessel and examine the probe for obvious signs of damage that may prohibit reprocessing (cracks, missing pieces, etc.). Confirm the soiled probe is compatible with reprocessing in Ethos.4-6 Obtain a single-use bottle of AquaCide and check that the disinfectant has not expired and the bottle’s integrity is intact.4. Automated Cleaning and High-level Disinfection (HLD):
Ethos uses automated cleaning and HLD to minimize operator hands-on time and human errors.a. Starting a Cycle: Follow the prompts on the Ethos display to insert the probe and record run information. Insert the AquaCide bottle into Ethos, shut the door, and the cleaning and disinfection cycle will begin.

b. Cleaning and Disinfection: Ethos automatically cleans, high-level disinfects, and rinses the transvaginal probe using the FDA-cleared concentration and exposure time for AquaCide. Disinfect cables/cords using a compatible low-level disinfectant.4 The cables can be disinfected while the automated disinfector is running. Once the cord has been disinfected, the operator can walk away until the cycle is complete. Remove gloves and wash hands after handling the contaminated probe.7 Discard gloves as biohazardous waste.
c. Automated Chemical Indicator System: During the cycle, the cleaner/disinfectant is automatically tested using the QwikCheck chemical indicator to determine if the active ingredient concentration is above the minimum recommended concentration (MRC). The multi-use QwikCheck chemical indicator bottle can be stored at room temperature, and is attached inside Ethos on its built-in shelf. The Ethos also automatically tracks chemical indicator liquid levels and expiration dates to prevent usage of expired indicator or insufficient indicator volume.
5. Cycle Completion and Drying:
Don appropriate PPE (e.g. clean gloves and eye protection). Check that the cycle is complete, and the Ethos encountered no system errors, as evidenced by a printed ticket stating that the run “Passed.”a. Passed and Complete Cycle: Following a successful cycle, remove the probe from the automated disinfector being careful not to contaminate or damage the probe.
b. Failed or Aborted Cycle: In the rare event that the system detects a run abnormality, the run will abort and automatically rinse the probe using fresh water. A “failed” report ticket will be automatically printed and should not be discarded. The probe is not considered disinfected and should be handled accordingly.
c. Drying: Once removed from the Ethos, dry the probe thoroughly using a gamma-irradiated, single-use lowlint cloth; starting at the lens and working toward the handle and cord. Do not use any drying cloth with compromised packaging or that is visibly soiled. For drying cloths that are not individually packaged, make sure that cloths were properly stored (i.e. in a closed, sealed container) to avoid environmental contamination. Drying cloths that were improperly stored (i.e. open to the environment for an extended time) should not be used. While drying, inspect the probe for any residual soil or damage. Place the dried probe in a clean probe storage cover.

Removing rinse water using a gamma-irradiated drying cloth
6. Storage:
Probes should be clearly labeled with the storage date, level of disinfection (e.g. HLD), and maximum storage duration according to institutional policies.4 In some facilities, probes may need to be transported to another storage location. Covered probes should be handled and transported in a manner that prevents contamination.4 Store probes in probe storage covers or cabinets with high efficiency particulate air (HEPA) filtration to reduce the risk of re-contamination from the environment. Do not place dirty and clean/disinfected transducers in the same cabinet or probe storage cover.4 Unless otherwise specified by the manufacturer, only one probe should be stored in each probe storage cover.
HEPA-filtered dedicated storage cabinet for cleaned and high-level disinfected ultrasound probes
7. Documentation and Traceability:
At the end of each run, a ticket containing the relevant run information, such as model, serial number, reprocessing personnel, validation result (e.g. chemical indicator information, temperature, disinfection time), lot numbers, and date/time is printed. Documentation can be completed using manual or automated processes.4 Printed tickets can easily be maintained using the Ethos Log Book. Run information is also stored on a USB drive for uploading to electronic systems.8. Hand Hygiene:
Remove PPE and discard appropriately. Wash hands before proceeding to next task.6Ethos is the first FDA-cleared automated system for cleaning and high-level disinfecting transvaginal or transrectal ultrasound probes. The fully automated workflow eliminates many of the potential issues associated with manual and semi-automated reprocessing methods. Ethos is an enclosed system, which helps contain disinfectant fumes to protect staff and eliminates the need for bulky and costly fume hoods and enclosures. The Ethos workflow also requires the least amount of operator handson time, when compared to the manual and semi-automated methods. This combined with the automated sampling and reading of the chemical indicator provides a completely hands-free process from the cycle start to end. Clinical staff and reprocessing technicians can then be available to focus on completing other tasks. Further, the automated workflow also addresses the issue of human error associated with both the manual cleaning and HLD procedures, while eliminating potential variability between operators. With a single automated workflow for multiple probe models and manufacturers, Ethos represents the next advancement in transvaginal and transrectal ultrasound probe reprocessing procedures.

Proper cleaning and disinfection of transvaginal and transrectal probes is essential to providing a safe patient environment and preventing healthcare associated infections. Developing and following procedures in accordance with current best practices and guidelines can help reprocessing staff work safely and efficiently without compromising patient safety. A completely automated cleaning and disinfection of transvaginal and transrectal probes in CS Medical’s Ethos automated ultrasound probe cleaner disinfector provides some distinct advantages. Automated workflows are safer for staff by preventing chemical exposures and for patients by reducing the likelihood of human error to provide a reproducibly, and reliably clean and disinfected probe each time. Further, the ability to use a single reprocessing workflow for compatible probes from different manufacturers can reduce confusion and time spent checking reference materials for each individual probe. Clinical staff and reprocessing technicians have more hands-off time during the automated reprocessing procedure to complete other clinical tasks to maximize their time. The result is a single, efficient, and reproducible workflow that promotes patient safety and infection prevention in healthcare settings.
References
- The Joint Commission, Quick Safety Issue 33: Improperly sterilized or HLD equipment - a growing problem. 2017.
- The Joint Commission, Top 5 Most Challenging Requirements for 2022. 2023, The Joint Commission Online.
- Carrico, R.M., S. Furmanek, and C. English, Ultrasound probe use and reprocessing: Results from a national survey among U.S. infection preventionists. American Journal of Infection Control, 2018. 46(8): p. 913-920.
- Society of Diagnostic Medical Sonography, Sonographer Best Practices for Infection Prevention and Control: Reprocessing the Ultrasound Transducer. 2022: Plano, TX.
- Rutala, W.A., D.J. Weber, and Healthcare Infection Control Practices Advisory Committee, Guideline for Disinfection and Sterilization in Healthcare Facilities, , Centers for Disease Control and Prevention Editor. 2008. p. 14-21. Medicine.
- American Institute of Ultrasound in Medicine, AIUM Official Statement: Guidelines for Cleaning and Preparing External- and Internal-Use Ultrasound Transducers and Equipment Between Patients as Well as Safe Handling and Use of Ultrasound Coupling Gel. J Ultrasound Med, 2023. 42(7): p. E13-E22
- American College of Emergency Physicians, Guideline for Ultrasound Transducer Cleaning and Disinfection. 2021.
- Food and Drug Administration, Reprocessing Medical Devices in Health Care Settings: Validation Methods and Labeling, Center for Diagnostic and Radiological Health. 2017.
- Johnson, S., et al., Evaluation of a hydrogen peroxide-based system for high-level disinfection of vaginal ultrasound probes. J Ultrasound Med, 2013. 32(10): p. 1799-804.
- Lambert, R.J. and Johnston, M.D., The effect of interfering substances on the disinfection process: a mathematical model. J Appl Microbiol, 2001. 91(3): p. 548-55.
- Rutala, W.A. and Weber, D.J., Uses of inorganic hypochlorite (bleach) in health-care facilities. Clin Microbiol Rev, 1997. 10(4): p. 597-610.